
TRANSCRIPT:
(This transcript is derived from an automated process. The video recording is authoritative.)
Gary Johns:
Thank you, Jewel and especially all the work you do to allow people like myself and Kevin to speak to you sometimes at length and sometimes shorter about the work we've done over many years. You need hundreds of these sort of forums around the country to get a message out and that's what we're prepared to do. We'll just keep yapping away and I'm sure at some stage we'll hit gold.
Anthony Capello tells me the books are selling at $30 tonight rather than 40 because they're not posted and I don't actually have a copy of the book. There's literally hot off the press. So it's all brand new.
Now we set out, this is an update of a book that I published in 2017 and Anthony suggested I update it post COVID because so much of the COVID response driven by public health officials was so bad that we thought we should write some more about it.
The book's not just about COVID, it's about a mindset, a conceit on the part of public health officials. So let me sort of take you into the heart of public health them and see what it means. Now what is it?
Public health according to our friends at the United Nations is really about something that is socially determined and that public health is about people's access to power and money and resources, which of course are inequitably spread around and that's got to be unfair, but it's avoidable. So immediately health is lifted into another level and it becomes a social and political event which suits the socialist mindset precisely.
So we argue that the public health lobby is driven by ego and ideology.
The ideology of course is a socialist one that if we can just spread the money around enough, everyone will live as long as everyone else. And the ego is driven by the medical side of public health that says we are powerful and we are knowledgeable.
Put those two together and you get a drive that says no stone is to be left unturned to help even those to better health who didn't even ask for it, which is what happened in COVID.
Now I thought I should give you an example of someone who's not a public health official, but who certainly looks like one and sounds like one, thinks like one. Dr. Monique Ryan, MP, a member for Kooyong who beat Josh Frydenberg at the election before last and survived at the last election.
She is or was practising as a paediatric neurologist and an extremely gifted and intelligent woman. What has she done with that gift? Wasted it. She should never have left the medical profession. Instead, this is what's on her website today.
"Heat waves are Australia's most deadly climate hazard responsible for more deaths than extreme floods", et cetera, et cetera, et cetera.
So she wants to name each heat wave. Why? So that we'll be afraid of climate change.
So there's an extremely intelligent, highly educated person, a paediatric neurologist telling us crap that somehow heat waves of which there've been a lot in Australia are responsible for deaths.
Well, heat waves at the margins are responsible for deaths unless of course you have good air conditioning, which is driven by coal, gas and oil.
She wants to destroy our ability to protect ourselves from heat waves and her antidote is to name the heat wave in support of an ideology that says we can turn down the temperature of the earth.
Now, if you're a clinician in the hospital, I think you can apply wet press and certain chemicals to lower the temperature, but for the earth, give it a break. This is the sort of person who destroys the good name of medicine and destroys good public policy. So we'll keep her in mind as we go through.
Now public health officials make all sorts of errors and in the book we've sort of picked out seven major errors. Kevin referred to some of these and we'll just pop through them.
First of all, as the public health officials discount DNA as the main determinant of health, they say, "No, it's an external thing. It must be social injustice. It must be because you don't have enough money. I can tell you the best science says it's DNA. Your mom and dad determined most of your health outcomes."
Now that's not a sentence one way or the other. It just means the ability to intervene in your health is a lot narrower than public health officials point out.
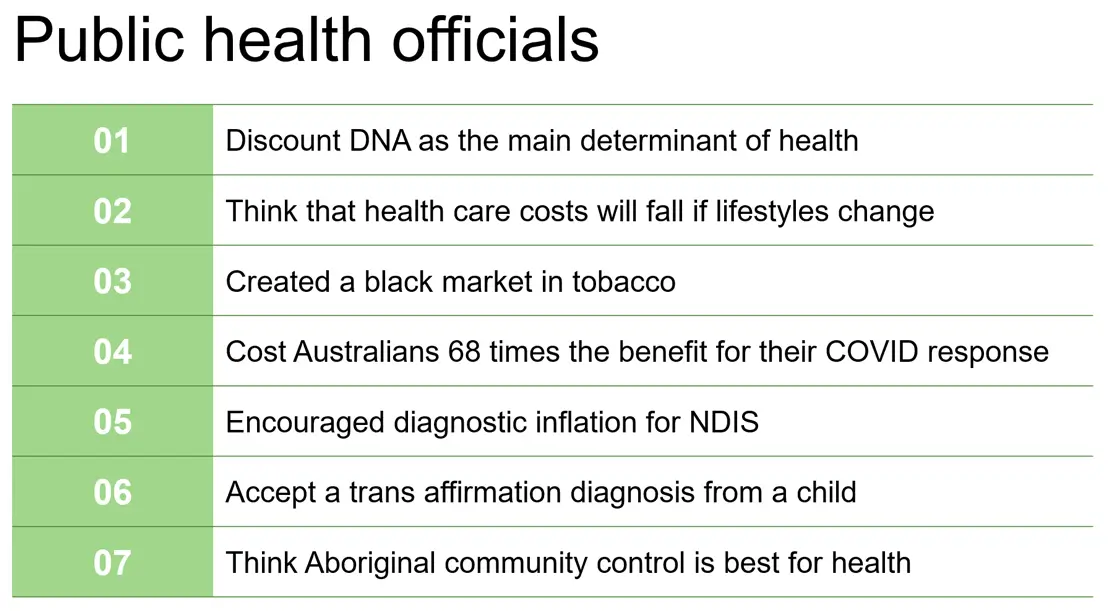
Second one, they think that healthcare costs will fall if lifestyles change. They're wrong. They always come up with big dollars. We can save society money by X. We'll give you an example where they're not saving money at all.
They're costing us. The other one is they've recently created a black market in tobacco because when professors in their white coats go to the politician and say that we must stop the tobacco industry, the politician is told that the one way to do it is to put an excise, a tax on tobacco sales and then the silly blighters keep doing it.
Both governments, Scomo and his time put up the tax on tobacco 12 and a half percent year on year on year. This mob's only putting it up 5% or whatever. But I shop at Coles and I see the poor blighters who still buy cigarettes. They're about 10% of Australians and they are the poorest Australians and they're being made poorer by this.
But criminals see a market opening because there's such a difference in price between the tobacco products sold legally and chop chop or illegal tobacco products imported that the market has opened up a black market.
And there are those who are arguing that we should lower the excise on tobacco so that the market is less productive, but there are about a dozen professors of health around the country who got together and said, "No, no, no. We don't give into that sort of nonsense. We want zero tobacco." They're not happy with 10% smoking in the country. They want zero.
So they want to actually improve the black market for a criminal market, criminal people.
Number four, you've had so much on COVID, but one of the best studies here in Australia is that the COVID response cost Australians 68 times the benefits. Canadian study has it, I think, at 140 times the benefits, but we won't go into that here because you've done enough of that.
Public health officials have encouraged diagnostic inflation in the NDIS. So in fact, it's at least 20 years now that the notion of neurodiversity, autism, and so on was written in a way that was almost nonclinical. It was almost advisory so that as soon as there was some money on the table so that your child might fit this broader category, you chase the money.
So half of the people today going on to NDIS have autism, ADHD, and the government is scrambling to get them back off.
You know what that means? There'll be another packet of money to look after those kids. They will not deny the diagnosis because that's medical and politicians are too afraid to touch that.
So in addition to the NDIS, you'll get what appears to be a narrowing, some savings in NDIS, but there won't be net savings. The rest of the money will go somewhere else.
And there's a negotiation between the states and the commonwealth as to who will pick up the bits and pieces. But thank you public health officials and other people who've allowed NDIS to grow by picking up people who are not really ill.
Next one, and of course you heard last month or whatever from Gillian Spencer, what a wonderful woman she is, what a brave person she is. And to sum it up, public health officials have said a child who probably has a mental health condition comes into your clinic and says, "I want to be transitioned."
And the doctor says, "That's a diagnosis. That's a beauty. We'll run with the pre-prescribed diagnosis of a mentally ill child." That's never been done before. It's normal that you go and you describe your symptoms and the doctor says, "Well, that could be X or Y."
You don't believe the patient for the diagnosis, only for the recognition of the symptoms, but that's what's happened. That's precisely what's happened in the trans afirmation thing. Leave that alone because Jillian is the expert.
The last one where I probably have a little bit of inside information is that there's been enormous growth in the last 30 years of Aboriginal community controlled health services. I visited many of them.
You visit a medium sized town in Australia, there'd be one or two outlets there and I've been to lots and there aren't many people in them. I don't know where the patients are, but what I can tell you is they are run by an Aboriginal family, usually the top family, and they appoint CEO or the chair and they're paid and all of the staff are non-Aboriginal medical staff.
The only Aboriginal staff have administrative positions. So if you substituted them with non-Aboriginal administrative positions, your outcomes would be precisely the same. There is no benefit or very little in having Aboriginal controlled community health services and the various lobbies of the Aboriginal community controlled health services keep telling us about two or three studies that prove that they're better.
I've looked in great detail excessively of the two or three studies, they don't say that at all. They don't even pretend to say that. So big fat lie, we're spending more money than we should otherwise do to have people stay at around about the same ill health for other reasons.
Okay. So you've got to be fair about this. I do try to put this in context and it's picking up Kevin's theme here. The context in which our heroes of public health ply their trade. The fact is because we are a wealthy society, we have since the introductory to Medicare and its elements of socialism and I'm for Medicare, go to the doctor more often. We used to go about four times a year. We now go about seven times a year.
We also use other services, physios. I live at the physio. So physios, podiatrists, all that sort of stuff. So we're using more medical services. So I want to distinguish that from public health.
There's no doubt that we crave to be well and we do have a lot of faith in medical science and we do go to the doctor a lot. Now there might be some false negatives in there that we shouldn't be, but there it is we do. This is a bit complex. Are we better off as a result of going to the doctor more and all of the medicine? Well, we are, but there's some trade offs here.
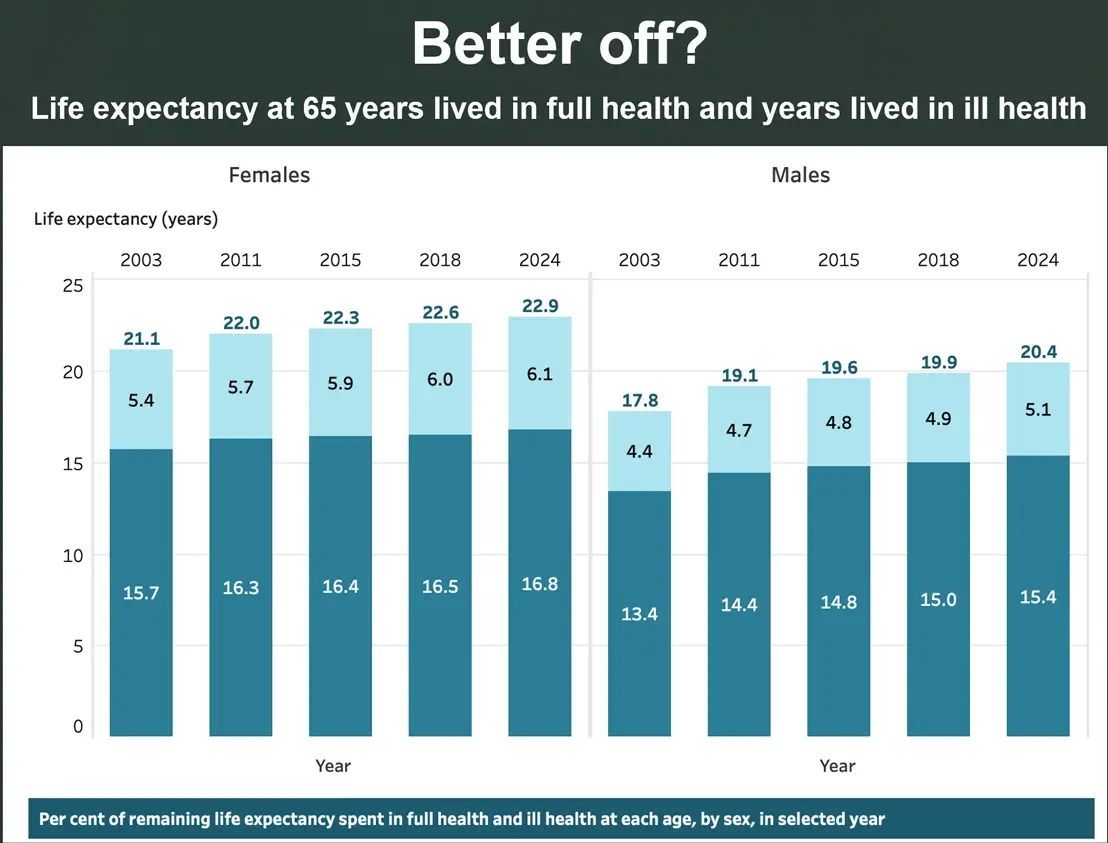
On the left it talks about females. On the right, it talks about males. Women for some reason live longer. I wonder if a man who wants to transition as a woman to a woman will get better outcomes.
Something to think about.
However, for a person at 65 years of age in 2003, you were said to live another 15.7 years in good health and 5.4 years in ill health. Combined, you'll live another 21.1 years. 65 year old person in 2024 lives a little longer, but lives longer in ill health. Not saying that's good, bad, or indifferent, but we have learned to keep people alive longer in good health as well as ill health.
That's pretty much what's driving the massive increase in costs in medicine. And it's not a moral judgement here, but there is a downside and I'll come to that when we get to public health. So you have to say, you have to put this critique of public health in context.
Now, the fact is that our health is pretty much determined by our DNA, particularly our brains and our personality. In nice language, cognitive ability and personality are the best predictors of health outcomes.
Now, if you look at an example here of an elderly person with chronic ailments who visited a GP more than 50 times in a year, 85% of whom are on welfare, you found that 40% failed to take their medication. So brilliant pharmacology comes to nothing because people failed to take pharmacology, their medicine.
And the only advice I've found in all of the research we've done about how you can get people to, if you like, change their behaviour sufficient to get the benefits of pharmaceutical medicine, other medical interventions, is to follow smart people.
See what a smart person does. Do they take their medicine? Do they look after themselves? Well, that's what you have to do, but not everyone can do that or wants to do that. And to compensate for those failures, we spend billions of dollars thinking we can intervene in a way that will overcome cognitive ability and personality.
So that's the sort of ground under which you need to ... That's the base. We need to understand that and then we can say, what added value does public health create? Simple answer, bugger all, but I mean, I'm trying to be nice and get there slowly.
So the opportunity for interventions narrow. Now it doesn't mean that medicine shouldn't try. I submit, I don't think I'd be here without some good interventions in medicine, but only where there's a direct relationship between cause and effects.
So Monique Ryan has this quite indirect relationship between storms and death, like really that is so indirect it's highly unlikely that naming storms or even somehow trying to stop them by whatever it is she thinks might stop them will have a significant effect on the lives of people. So it's rare in typical public health campaigns such as obesity or climate change that there is such a direct effect, but by golly, they invent some big numbers.
This is the game. In public health, you have to generate big numbers and big scares, which is what we saw during COVID, completely inflated, unrealistic, untrue numbers about the millions that were died, blah, blah, blah, blah, from all with COVID.
And you'll recall that if you deducted the people 85 years of age and older who died with or from COVID, there was no pandemic. There simply wasn't a pandemic and those are public figures I think published by the Australian Institute of Health and Welfare. Sorry. And a lot of the stuff, the numbers which deceive us are based on bad analysis.
So we're going to give you a really good little one.
Now the smoker scenario, this is the poor blighter he turns up at Coles and I see them take that packet of cigarettes out of the Coles work out of a non-named sliding door and pay over, I don't know, $50, $65 or whatever the extraordinary amount of money is, most of which is tax.
Now take this person. A long-term smoker may die of coronary heart disease at age 65. Now if he quits at 40, he may live until 75 and then die of chronic heart disease. The cost of treatment hasn't been avoided, it's just been postponed.
I'm not saying that's not a bad thing for that person, but in terms of public health, there's no difference. You're going to get the bill. It'll just come somewhat later. Now the savings from improved health before age 65 because the person gave up at 40 are offset by increased healthcare spending among people 65 and older.
So remember that graph I said increasing years of health and increasing years of ill health. So we're really unable to avoid that scenario of huge costs towards the end of life and an increasing years of ill health. The other one is the lost revenue. This maker paid no tobacco tax during the quitting period, so he wasn't going to pay for his ill health.
And you do know that the Commonwealth now receives, I think it's about half the revenue they used to receive from the tobacco tax because of the black market. And the other one too is that the reform smoker receives an age pension for additional 10 years, which he would not otherwise have received.
Now, I'm not saying smoke your self to death and go early. I'm not saying that. But if you really want to be fair to income about the public or the cost to the public of all these interventions, you have to have all of the figures in there. There are no savings in this.
It's good per individual to intervene to try to stop them to smoke, but when you go too far, you have a black market. And if you kid yourself that there's a saving to the public, you're just wrong.
Here's another little one. Recently the US is surgeon general, I think is the term, said that you must ban alcohol advertising. Now if, and here's an example of how it just won't work. So consuming alcohol may raise the relative risk of breast cancer by about 10% per standard drink per day. That's the relative risk, but you have to think of the absolute risk. The absolute risk of a woman in her 40s developing breast cancer over the next decade is 1.5%. If she has one glass of wine daily, that's a 10% rise in the relative risk as we were told, but the absolute risk climbs just 1.65%.
So if you compare a thousand women who don't drink with a thousand who drink one glass of wine each day, there are 15 non-drinkers who'll develop breast cancer over the next decade, but that rises to just 16.5 drinkers. That's just one and a half cases in a thousand. That's not 10%. So you have to look at the actual incidence of an intervention.
The surgeon general says, stop the advertising because, and she will pick out a big number, 10%. The real number is a fraction of that. And then of course, where's the proof that banning the advertising of alcohol will stop a person having the extra drink? There's very little. So it's not just 1.5 cases extra. It's probably even less than that.
So public health officials confect scenarios. Can't say lie because you're not allowed in parliament, is it? No. But they confect scenarios that look really scary and really big as an excuse for them to intervene in a way that won't be effective because most people don't take their medicine.
Okay. Gary, terrific mate, but what are you going to do about it? And here's, I think, an insight which a few others have had.
Our bottom line is, can you let people do their job? Let the medicos do their job. That's where we failed in COVID. Individual doctors should have been talking to their patients without some person in China, then the UN and then the Commonwealth, that's how it went, telling us what we should do, the lockdown, et cetera, et cetera. Whereas many, many doctors would have given much more sensible views on that.
So what's happened is that if you go to the medical codes of ethics, these are being used as Trojan horses by public health to undermine the medical profession in a pursuit of progressive ideology. And so I had a look at the nurses ethics.
This is the International Council of Nurses Codes of Ethics. A woman who sits above this is in fact a former national president of the ACTU so you know where this is coming from, but it's also the Australians, the Australian nurses medical ethics.
So hang on, what should a nurse do? Be highly trained and looked after the person in front of them. That should be the ethic, but I know there's a lot more they have to do. They have to quote unquote, work towards achieving the United Nations sustainable development goals.
So as you're putting the old, what is it, a cannula or something in? Sustainability. Oh geez, sorry. A bit too much in there. Didn't keep your mind on the job, but that's what nurses are told. Recognise the significance of the social determinants of health. In other words, rather than take the person diagnosed and give them the correct medicine, you might distinguish between whether they're a rich or poor person or black or white or gay or straight, irrelevant to the medical question at hand, to collaborate, to protect the natural environment and what is it?
Are aware of the health consequences of environmental degradation, i.e. Everyone knows you're talking about climate change and we're back to the member for Kooyong, complete misuse and abuse of medical knowledge. What's the last one? Uphold justice by promoting responsibility in human rights, equity, fairness, blah, blah, blah, the public good and health and a healthy planet.
This is a misdirection of good medicine and there are a number of doctors who are being sued at the moment by, sued is that the right word, by AHPRA.
I'm looking at the Dr. Kok down in Melbourne and I've been reading the judgments and I'm thinking, what is the basis on which they can get stuck into Dr. Kok then? And they go to the code of ethics for doctors, for GPs.
There's nothing in the law. There's just one word in the law that says something like, "You should be ethical." What does that mean? They drop down to the doctor's codes of ethics and the doctor's codes of ethic have got all that nonsense sitting in there and that's what enables APRA at the medical board to make judgements about a person's political views. That's bad.
It does mean that if you want to fight this beast, you have to actually get the professions involved. And I think bottom line is we've got 10 things we ought to be doing, but I'll just go to this one.

The professions have to reclaim science and not play politics. I think what's happened over many years now is professionals are becoming more and more specialised. I did ask a very senior psychiatrist just recently, very good man, very bright, very experienced and conservative what he thought about the problems that Jillian Spencer was having and he sort of dropped his head and said, "She's in a world of pain."
I was expecting more of him. I was expecting him to say, "I should go to the College of Psychiatrists and fight this."
So I'm not blaming him, I'm just saying I think there are too many medical professionals who are just worried about their own little part. Someone AusPATH or whatever gets into of the profession, run by a non-medical CEO probably and lots of HR people who say, "Oh, this has been nice to play with. Why don't we have a whole code of ethics given to us by the UN?"
And the profession is hardly aware of it because it doesn't affect them day to day except when it does and now it's popped out in the trans affirmation issue shockingly, embarrassingly and damagingly for young men and boys and girls.
I think we've sort of found one of the key elements here in the fight back. There are nine others in the book. I'm not going to tell you tonight until you buy the book and ask me questions. Thank you very much. Thank you so much.



